
{kind=link}
{kind=link}
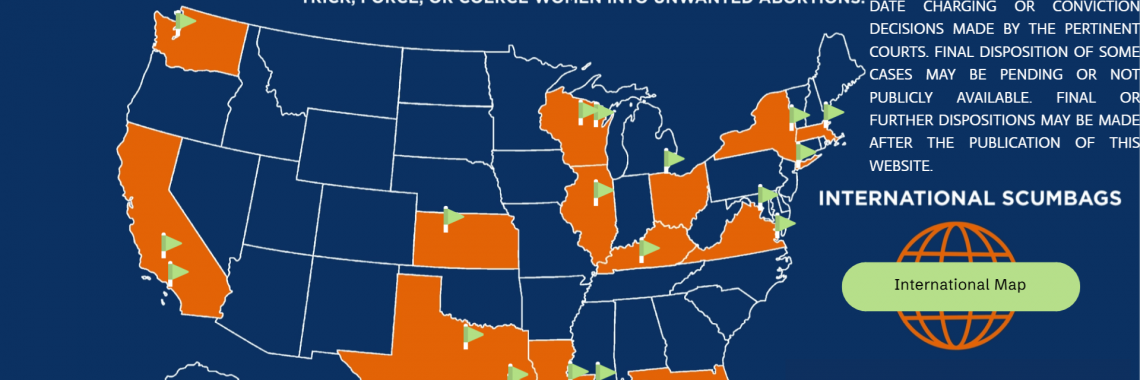
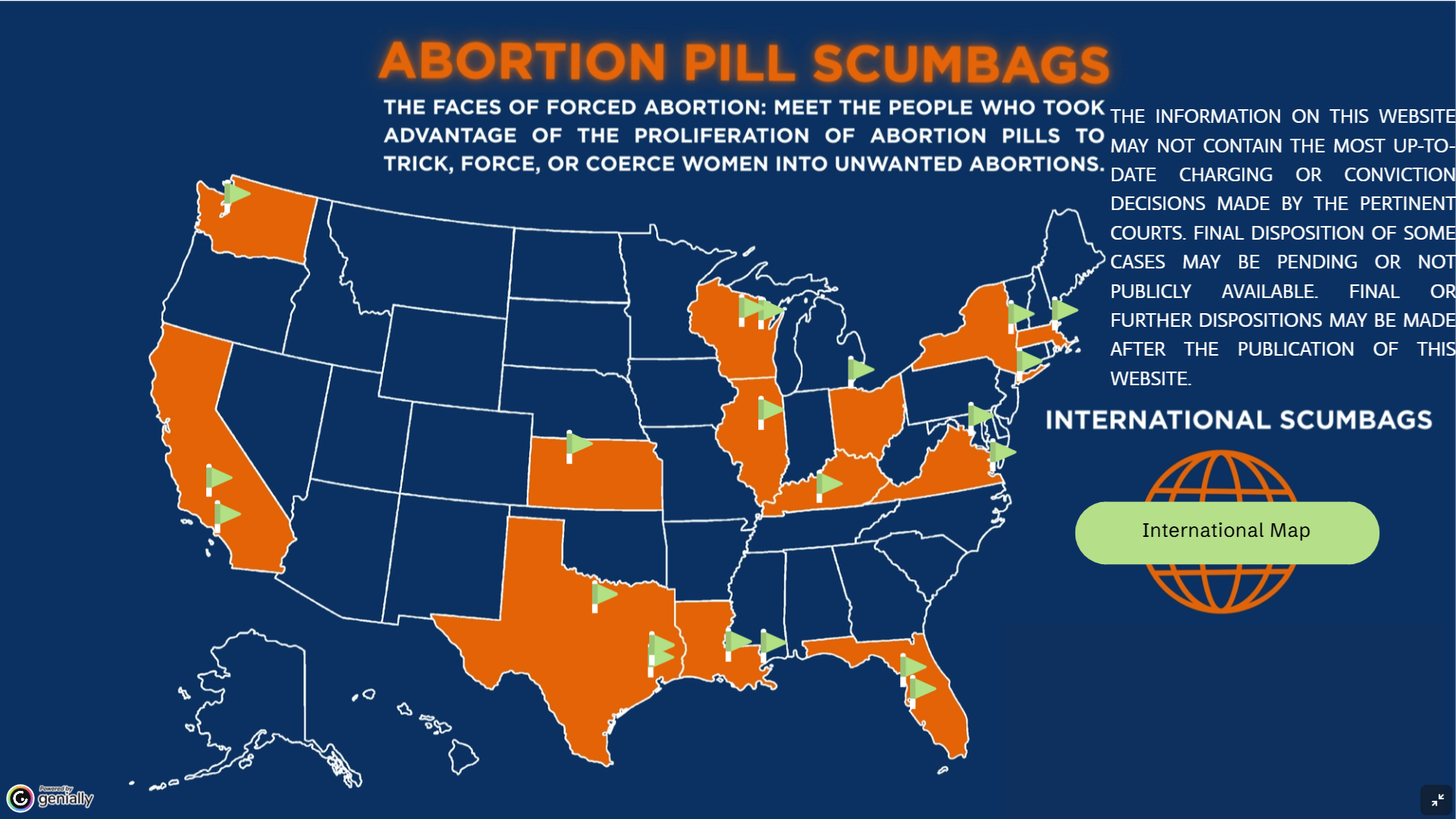
Pro-Life Group Highlights Abortion Pill Horror Stories
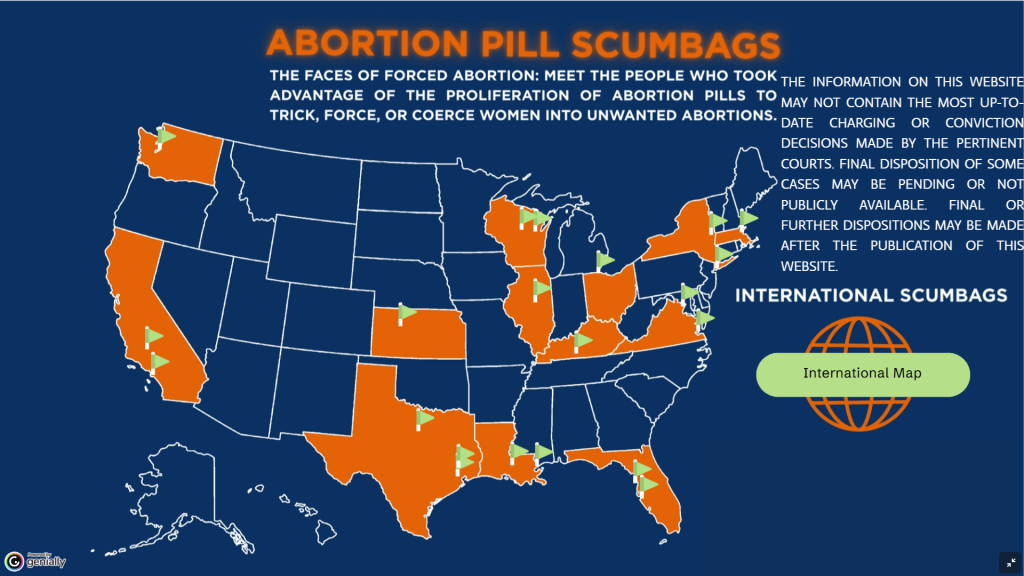
A Texas-based pro-life group has produced a list of abortion pill horror stories from across the nation.
The U.S. Food and Drug Administration first approved abortion drugs like RU-486 nearly 26 years ago, and in 2022 the agency loosened its safety protocols to make the drugs available by mail. But a recent study by the experts at the Ethics and Public Policy Center found abortion drugs are much more dangerous than policymakers previously thought. Since becoming available by mail, we have also heard stories about women coerced into taking abortion drugs or being given the drugs secretly, without their consent.
Pro-life organization 40 Days for Life has produced a summary of some of those stories.
For example, the group says a Kansas man “was sentenced to nearly a decade in prison for conspiracy to commit murder following allegations that he sprinkled a crushed abortion pill on his girlfriend’s pancakes to cause an abortion.”
In another case, the group says a Texas man was charged with slipping abortion drugs into mistress’s coffee and cookies.
A California man was sentenced to nine years in prison after drugging his pregnant girlfriend and then administering abortion drugs to her.
The entire list of stories is available at 40daysforlife.com/scumbags.
As we have said many times, abortion drugs are dangerous. They hurt women, and they kill unborn children. They should not be available at all — much less through the mail.
That’s why Family Council has joined with other groups to oppose these dangerous drugs.
In May, Family Council sent a letter to the U.S. Attorney’s Office for the Eastern District of Arkansas respectfully asking the office to enforce federal law as it applies to mail-order abortion drugs.
In June, Family Council joined a coalition of 83 state and national pro-life leaders urging acting U.S. Attorney General Todd Blanche to stop mail-order abortion drugs.
We have also partnered with pro-life organizations in an amicus brief asking a federal court to block mail-order abortion drugs nationwide.
In June, we launched a grassroots effort in Arkansas calling on the Trump administration and members of Congress to end former President Joe Biden’s dangerous mail-order abortion policies and restore the FDA’s safety protocols.
Arkansans can ask their members of Congress to oppose mail-order abortion by going to abortioncrimebymail.com
Articles appearing on this website are written with the aid of Family Council’s researchers and writers.

{kind=link}
Family Council Joins Coalition Urging U.S. Attorney General to Stop Mail-Order Abortions

Last week, Family Council joined a coalition of 83 state and national pro-life leaders urging acting U.S. Attorney General Todd Blanche to stop mail-order abortion drugs.
Arkansas law generally prohibits abortion except to save the life of the mother, and it is a crime for an abortionist to mail abortion drugs like RU-486 into the state.
But under President Biden, the U.S. Food and Drug Administration loosened its safety protocols to allow mail-order abortion drugs. Pro-abortion states have also enacted “shield laws” for abortionists who mail abortion drugs into states like Arkansas.
To make matters worse, the U.S. Department of Justice has opposed federal court cases from pro-lifers who want to to stop mail-order abortion.
All of this has created a dangerous industry of abortion-by-mail both in Arkansas and across the nation.
The letter to acting Attorney General Blanche asks him to “stop defending the abortion drug industry’s unlawful mail-order regime,” saying in part,
“Pro-life states cannot enforce their laws while an FDA regulation gives cover to mail-order abortionists and DOJ defends the profits of abortion drug manufacturers. The current regime undermines state laws, including basic protections against practicing medicine without a license, while shield-law abortionists ship drugs across state lines with impunity.”
Earlier this month, Family Council also joined a coalition of 57 pro-life organizations in an amicus brief asking a federal court to block mail-order abortion drugs in America and launched a grassroots effort in Arkansas calling on the Trump administration to end former President Joe Biden’s dangerous mail-order abortion policies.
Arkansans can join that grassroots effort at abortioncrimebymail.com.
New evidence shows that abortion drugs are much more harmful than the FDA previously thought.
A recent study by the experts at the Ethics and Public Policy Center found abortion drugs are at least 22 times more dangerous than the drugs’ labeling indicates. Nearly 11% of women experience serious health complications from abortion pills — including sepsis, infection, and life-threatening hemorrhage.
A recent Federalist poll found that 67% of likely voters support reinstating the in-person doctor’s visit requirement for abortion pills — including 63% of Democrats and 72% of Republicans. This is plain common sense, and Americans across the political spectrum agree.
Abortion drugs are dangerous. They hurt women, and they kill unborn children. The U.S. Department of Justice needs to recognize that fact and stop preventing states like Arkansas from enforcing their laws against mail-order abortion.
Articles appearing on this website are written with the aid of Family Council’s researchers and writers.